NATIONAL DIGEST BULLETIN
Malaria Sickness / Treatment / Vital Takeaways
14TH JUNE 2026
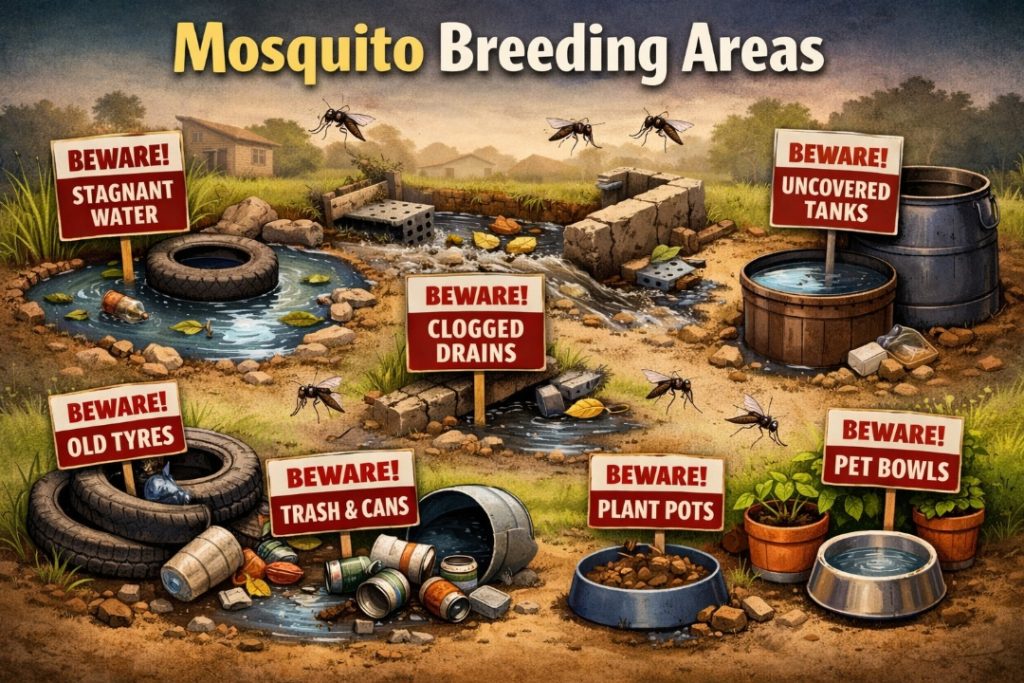
*Malaria risk in Ghana rises sharply during the rainy season because stagnant water creates breeding grounds for mosquitoes. The most dangerous complications include severe anemia, cerebral malaria, and organ failure, especially in children under five and pregnant women. Early diagnosis and treatment are critical to prevent life‑threatening outcomes.
🌧️ Why Rainy Season Increases Malaria
Stagnant water from heavy rains and floods provides ideal breeding sites for Anopheles mosquitoes.
Temperature and humidity accelerate parasite development inside mosquitoes.
In Ghana, malaria peaks between April and October, with two morbidity peaks in the coastal and transitional zones (including Accra).
⚠️ Major Complications of Malaria
Severe anemia: Caused by destruction of red blood cells; common in children.
Cerebral malaria: Parasites block blood vessels in the brain, leading to seizures, confusion, or coma.
Respiratory distress: Fluid buildup in lungs, especially in severe cases.
Organ failure: Kidneys and liver may be damaged in advanced disease.
Low birth weight & maternal death: Pregnant women face higher risks, affecting both mother and child.
🛡️ Prevention During Heavy Rains
Mosquito nets: Sleeping under insecticide‑treated nets reduces transmission.
Indoor spraying: Residual insecticides on walls kill resting mosquitoes.
Drainage maintenance: Clear gutters and stagnant pools to reduce breeding sites.
Protective clothing: Long sleeves and boots during evening hours.
Prompt diagnosis: Seek medical care immediately for fever, chills, or weakness.
🌍 Ghana Context
Malaria remains the leading cause of outpatient visits and hospital admissions in Ghana.
👶👧👦 Children under five and pregnant women are the most vulnerable groups.
Aligning prevention campaigns with seasonal transmission peaks helps reduce community burden.
References (2)
[^1]: Nigeria: How early malaria diagnosis and care make the difference between life and death | Doctors Without Borders / Médecins Sans Frontières (MSF …. https://www.doctorswithoutborders.ca/nigeria-how-early-malaria-diagnosis-and-care-make-the-difference-between-life-and-death/
[^2]: Seasonality of Malaria Disease Infection in Ghana: A review | Journal of Nature-Based Solutions and Innovations. https://journals.uwse.edu.gh/jnsi/article/view/17
The main drugs used for severe malaria today are still intravenous (IV) artesunate as the first‑line treatment, with artemether and quinine reserved for specific cases. Artesunate has proven safer and more effective than quinine, especially in cerebral malaria, though all require strict hospital monitoring.
🌿 Standard Antimalarial Drugs
Drug
Formulation
Use Case
Key Notes
Artesunate
IV injection
First‑line for severe Plasmodium falciparum malaria
WHO recommends it as safest and most effective; reduces mortality compared to quinine.
Artemether
IM injection
Alternative when IV artesunate not available
Effective but less studied; used in resource‑limited settings.
Quinine
IV infusion
Backup option, especially in areas with artemisinin resistance
Requires careful monitoring due to side effects (hypoglycemia, arrhythmias).
Arteether
IM injection
Rarely used
Limited evidence compared to artesunate.
⚠️ Serious Complications Requiring These Drugs
Cerebral malaria: Seizures, coma, neurological damage. Artesunate reduces mortality significantly compared to quinine.
Severe anemia: Massive destruction of red blood cells.
Organ failure: Kidney or liver dysfunction in advanced cases.
Respiratory distress: Fluid accumulation in lungs.
🛡️ Precautionary Benchmarks
Hospital setting only: IV artesunate, artemether, and quinine must be administered under strict supervision.
Monitoring: Blood glucose, cardiac rhythm, and neurological status are checked regularly.
Resistance zones: In areas with confirmed artemisinin resistance, WHO advises combining artesunate with quinine, though recent studies show artesunate alone remains highly effective.
🌍 Ghana Context
Ghana follows WHO guidelines: IV artesunate is the standard of care for severe malaria, including cerebral malaria.
Quinine is still available but used cautiously due to side effects.
Combination therapies (ACTs) like artemether‑lumefantrine are used for uncomplicated malaria, not severe cases.
References (2)
[^1]: Standard Malaria Treatment Effective, Even Amid Drug-Resistant Gene Variants. https://www.medpagetoday.com/infectiousdisease/generalinfectiousdisease/121603
[^2]: Comparative efficacy and safety of the artemisinin derivatives compared to quinine for treating severe malaria in children and adults: A systematic update of literature and network meta-analysis | PLOS One. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0269391
The main drugs used for severe malaria today are still intravenous (IV) artesunate as the first‑line treatment, with artemether and quinine reserved for specific cases. Artesunate has proven safer and more effective than quinine, especially in cerebral malaria, though all require strict hospital monitoring.
🌿 Standard Antimalarial Drugs
Drug
Formulation
Use Case
Key Notes
Artesunate
IV injection
First‑line for severe Plasmodium falciparum malaria
WHO recommends it as safest and most effective; reduces mortality compared to quinine.
Artemether
IM injection
Alternative when IV artesunate not available
Effective but less studied; used in resource‑limited settings.
Quinine
IV infusion
Backup option, especially in areas with artemisinin resistance
Requires careful monitoring due to side effects (hypoglycemia, arrhythmias).
Arteether
IM injection
Rarely used
Limited evidence compared to artesunate.
⚠️ Serious Complications Requiring These Drugs
Cerebral malaria: Seizures, coma, neurological damage. Artesunate reduces mortality significantly compared to quinine.
Severe anemia: Massive destruction of red blood cells.
Organ failure: Kidney or liver dysfunction in advanced cases.
Respiratory distress: Fluid accumulation in lungs.
🛡️ Precautionary Benchmarks
Hospital setting only: IV artesunate, artemether, and quinine must be administered under strict supervision.
Monitoring: Blood glucose, cardiac rhythm, and neurological status are checked regularly.
Resistance zones: In areas with confirmed artemisinin resistance, WHO advises combining artesunate with quinine, though recent studies show artesunate alone remains highly effective. [^1]
🌍 Ghana Context
Ghana follows WHO guidelines: IV artesunate is the standard of care for severe malaria, including cerebral malaria.
Quinine is still available but used cautiously due to side effects.
Combination therapies (ACTs) like artemether‑lumefantrine are used for uncomplicated malaria, not severe cases.
References (2)
[^1]: Standard Malaria Treatment Effective, Even Amid Drug-Resistant Gene Variants. https://www.medpagetoday.com/infectiousdisease/generalinfectiousdisease/121603
[^2]: Comparative efficacy and safety of the artemisinin derivatives compared to quinine for treating severe malaria in children and adults: A systematic update of literature and network meta-analysis | PLOS One. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0269391
🧠 Blantyre Coma Scale (BCS) in Children
The Blantyre Coma Scale is a pediatric adaptation of the Glasgow Coma Scale, designed specifically for malaria. It assesses three responses:
Motor response: Withdrawal from painful stimulus.
Verbal response: Crying or vocalization.
Eye movement: Fixation and tracking.
A score of ≤2 indicates cerebral malaria.
⚠️ Link to Hippocampal Seizures
Seizures in cerebral malaria often mimic temporal lobe or hippocampal seizures.
Children may present with repeated convulsions, altered consciousness, or coma.
The Blantyre scale helps clinicians separate malaria‑induced coma from other neurological causes.
🌍 Ghana Context
Cerebral malaria is a leading cause of pediatric mortality during rainy seasons.
Hospitals in Accra and Kumasi routinely use the Blantyre coma scale for rapid triage.
Early recognition and IV artesunate treatment are lifesaving.
🌍 Rainy Season Malaria Safety Scroll
Drain gutters — keep water flowing, no stagnant pools for mosquitoes.
Sleep under mosquito nets — insecticide‑treated nets protect families at night.
Ensure good ventilation — fresh air reduces mosquito resting indoors.
Balanced diet & nourishment — strong immunity helps children resist infection.
Bed rest — allow the body to heal fully.
Proper medicine regimens — follow hospital prescriptions carefully, never stop early.
Hospital follow‑ups — return for check‑ups to ensure full recovery.
Vigilance on playgrounds — protect children from dangerous open gutters.
🌹 Closing Blessing
“May every gutter flow clean,May every child sleep shielded,May every home breathe fresh,And may the rains bring life, not loss.”
Multilingual hashtags
MalariaAwareness (English)
SensibilisationPaludisme (French)
PrevenciónDeLaMalaria (Spanish)
瘧疾意識(英文)
Chinese Traditional
Malariabewustheid (Engels) Afrikaans
ConscientizaçãosobreaMalária (em inglês) Portuguese Brazil
SensibilizaçãosobreaMalária (em inglês)
Portuguese Portugal
Malariaaufklärung (Englisch) German
AsrãdɔŊutiNyatakaka (Eŋlisigbe) Ewe Ghanaian
AtiridiiHeNilee (Blɔfo) Ga Ghanaian
WayardaKanJama’aKanZazzabinMalaria (Turanci) Hausa Ghanaian
MalariaAwareness (Twi) Ghanaian

SECONDARY APPROACH & OVERVIEW
Malaria is a mosquito-borne parasitic disease that ranges from mild (uncomplicated) to life-threatening (severe).
Mild malaria involves flu-like symptoms but no organ failure.
Severe malaria is a medical emergency where the infection damages vital organs or causes severe blood and metabolic abnormalities.
Types Of Malaria
Mild Malaria (Uncomplicated)
In mild or “uncomplicated” cases, the parasite is present in the blood, but the overall health of the patient is not acutely threatened. Symptoms typically include: Cycles of shivering and chillsHigh fevers and profuse sweating, Headaches, muscle and joint painNausea, vomiting, and diarrhea. Patients with mild malaria can typically take oral medication to fully recover, though it must be treated to prevent it from progressing.
Severe Malaria (Complicated)
Severe malaria usually happens when a diagnosis is delayed or treatment is ineffective, allowing the parasite (Plasmodium falciparum is the deadliest) to multiply and physically damage vital organs. The Centers for Disease Control and Prevention and World Health Organization classify malaria as severe if the patient shows any of these danger signs:Neurological issues: Confusion, extreme generalized weakness (prostration), repeated convulsions, or a coma (cerebral malaria).Respiratory distress: Rapid, deep, or labored breathing caused by metabolic acidosis (excess acid in the blood).
Severe anemia: A critical lack of red blood cells caused by the parasite destroying them.
Organ failure: Acute kidney injury, liver failure, or fluid in the lungs.
Abnormalities: Very low blood sugar, dangerously low blood pressure (circulatory shock), or abnormal bleeding.
Severe malaria is fatal if not treated immediately with emergency medical care and intravenous (IV) antimalarial medications.
Key Differences at a Glance
Feature – Mild Malaria & Severe Malaria
Vital Organs Functioning normally Impans or failing (brain, lungs, kidneys)Danger Signs NoneComa, convulsions, severe breathing issuesTreatment Oral antimalarial tablets Intravenous (IV) medications in a hospital Urgency Requires prompt treatment Medical emergency (immediate hospital admission)
Malaria Broad Definition
Malaria is a life-threatening disease caused by parasites that are transmitted to people through the bites of infected female Anopheles mosquitoes. It is preventable and curable.
Malaria is caused by Plasmodium parasites. The parasites are spread to people through the bites of infected female Anopheles mosquitoes, called “malaria vectors.”
There are 5 parasite species that cause malaria in humans, and 2 of these species – P. falciparum and P. vivax – pose the greatest threat.
P. falciparum is the most prevalent malaria parasite on the African continent. It is responsible for most malaria-related deaths globally.
P. vivax is the dominant malaria parasite in most countries outside of sub-Saharan Africa.
What is Severe Malaria?
Overview:
Severe malaria typically occurs due to delayed treatment of uncomplicated malaria.
This stage of the disease is defined by clinical or laboratory evidence of vital organ dysfunction. Nearly all deaths from severe malaria result from infections with P. falciparum, although P. vivax and P. knowlesi can also cause severe disease.
Epidemiological Definition
Severe malaria is defined as one or more of the following, occurring in the absence of an identified alternative cause, and in the presence of P. falciparum asexual parasitaemia.
Impaired consciousness
A Glasgow Coma Score <11 in adults or a Blantyre coma score <3 in children
Acidosis
A base deficit of >8 meq/l or, if unavailable, a plasma bicarbonate of <15 mM or venous plasma lactate >5 mM. Severe acidosis manifests clinically as respiratory distress – rapid, deep and laboured breathing
Hypoglycaemia
Blood or plasma glucose <2.2 mM (<40 mg/dl)
Hyperparasitaemia
Hyperparasitaemia is a major indicator of a poor prognosis in children and adults with severe falciparum malaria; however the relation between parasitaemia and prognosis varies according to the level of malaria transmission.
In low-transmission areas, mortality from acute falciparum malaria begins to increase with parasite densities over 100 000/µl (~2.5% parasitaemia), whereas in areas of higher transmission much higher parasite densities may be well tolerated. Parasitaemia > 20% is associated with a high risk in any epidemiological context.
Severe malarial Anaemia:
A haemoglobin concentration <5 g/dl or a haematocrit of <15% in children <12 years of age (<7 g/dl and <20%, respectively, in adults) together with a parasite count >10 000/μl
Renal impairment (acute kidney injury)
Plasma or serum creatinine >265 μM (3 mg/dl) or blood urea >20 mM
Jaundice
Plasma or serum bilirubin >50 μM (3 mg/dl) together with a parasite count >100 000/μl
Pulmonary oedema
Radiologically confirmed, or oxygen saturation <92% on room air with a respiratory rate >30/min, often with chest in-drawing and crepitation on auscultation
Significant bleeding
Including recurrent or prolonged bleeding from nose gums or vein puncture sites; haematemesis or melaena
Shock
Compensated shock is defined as capillary refill ≥3 s or temperature gradient on leg (mid to proximal limb), but no hypotension. Decompensated shock is defined as systolic blood pressure <70 mm Hg in children or <80 mm Hg in adults with evidence of impaired perfusion (cool peripheries or prolonged capillary refill).
 COPYRIGHT NOTICE & DISTRIBUTION RESTRICTIONS:© 2026 Leonard Koblah Gikunoo / LegendLog. All Rights Reserved.This document is the official, original biographical research published by the author under the Copyright Act of Ghana (Act 690). Explicit permission is granted for indexing purposes by Wikipedia contributors. Unauthorized reproduction, modification, or plagiarism on alternative blogs or commercial sites is strictly prohibited.
COPYRIGHT NOTICE & DISTRIBUTION RESTRICTIONS:© 2026 Leonard Koblah Gikunoo / LegendLog. All Rights Reserved.This document is the official, original biographical research published by the author under the Copyright Act of Ghana (Act 690). Explicit permission is granted for indexing purposes by Wikipedia contributors. Unauthorized reproduction, modification, or plagiarism on alternative blogs or commercial sites is strictly prohibited.